Report from the 4th International Scientific Congress on SMA
Report from the 4th International Scientific Congress on SMA
30th April 2024
Kim Kant-Smits (University Medical Centre, Utrecht, Netherlands), a paediatric physical therapist and PhD student, presented research looking into the impact of exercising the breathing muscles in SMA.
Weakness of muscles used for breathing (also known as respiratory muscles) can complicate SMA by impairing coughing and contributing to repeated infections of the airways. It can also result in breathing that is too shallow or too slow at night time, and can ultimately cause respiratory failure. There is therefore a great need for strategies to improve respiratory muscle function.
Dr. Kant-Smits presented a clinical study designed to assess the feasibility and effectiveness of respiratory muscle training in people with SMA Types 1 to 4. Known as the RESISTANT study, it was a single-blind and sham-controlled trial of a 4-month training period, followed by an 8-month extension phase. The personalised training programs could be completed at home and involved 30-breathing cycles using a respiratory muscle training device. Participants were asked to complete ten training sessions over 5-7 days per week.
The training device was set to provide resistance against breathing for those in the ‘training group’, and no resistance to those in the ‘sham-controlled group’. After 4 months, all participants were moved to the ‘training group’ for an 8-month extension.
Three children and 27 adults were included in the study, with the average age of participants being 38 years and all SMA Types being represented (three Type 1, 19 Type 2, seven Type 3 and one Type 4). At the time of study, seven participants were not receiving any SMN-boosting therapies, 17 were taking risdiplam, and six were receiving nusinersen.
After 4 months, the ‘training group’ successfully completed 62% of the training sessions and the ‘sham-controlled group’ completed 91%, and all participants scored the acceptability of the training as at least ‘good’ after this period.
There was no clear difference between the training and control groups in the strength of inhaling and exhaling. However, the ‘training group’ showed an average increase of 14.1% in inhalation strength compared to baseline, while the ‘sham-controlled group’ showed an increase of 9.6%. Exhalation strength was also increased by 4.9% in the ‘training group’ and 3.3% in the ‘sham-controlled group’. Participants self-reported improvements with the training, and those that completed more training sessions tended to have greater improvements in breathing muscle function.
Altogether, the study indicates that training of respiratory muscles is safe and feasible, and that there is the possibility that training has a positive effect on breathing muscle function in SMA. In the future, different training volumes and periods will need to be assessed in a larger group of participants to fully determine the impact of the training.
Channa Hewamadduma (University of Sheffield, UK), a consultant neurologist and honorary senior lecturer, presented findings from a new tool designed to assess bone health in adults with SMA.
People with SMA are more likely to have low bone mineral density, which means that they have a lower amount of important structural components within their bones. This makes bone issues such as osteoporosis and fractures / breaks much more likely across all SMA Types.
Dr. Hewamadduma and colleagues in a multi-disciplinary team designed an audit tool to assess bone health in people with adult SMA, and tested it with 53 participants who attend a regional SMA centre in Sheffield, UK. Detailed information from all participants was collected, including clinical symptoms, SMN gene and treatment information, chemical measures of bone health, bone density scans and information on any interventions conducted to prevent bone fractures.
There were 25 participants with SMA Type 2 and 28 with SMA Type 3, 13 of which were able to walk. The average age of those involved was 30 years, and 31 participants were receiving nusinersen and 22 were taking risdiplam.
Vitamin D is needed to regulate the amount of calcium and phosphate in the body, which are required to maintain good bone health. Vitamin D levels were low in 85% of participants in the study, and severely low in 60%. In non-white participants, vitamin D levels were on average lower than white participants, and all those with SMA Type 3 had low vitamin D. Three out of the 13 people able to walk suffered a bone fracture during the study that resulted in loss of ambulation (ability to walk).
This study highlights that there are clear bone health issues in SMA and that fracture prevention is important, as bone breaks can lead to loss of the ability to walk. The specially designed audit tool was clearly valuable for identifying bone issues and may be used at other centres to improve the management and understanding of SMA.
Hazel Allardyce (University of Aberdeen, UK), a postdoctoral scientist in the laboratory of Simon Parson, presented her latest work looking at the impact of SMA on blood vessels in the nervous system.
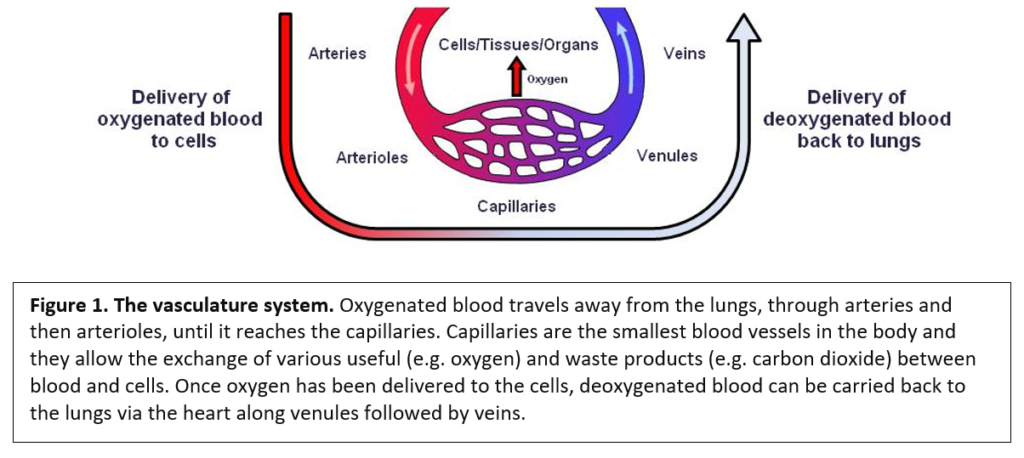
SMA was originally believed to be a disease that only affects the motor neurons, which are the cells that connect the brain and spinal cord with our muscles. However, over the last decade or so, increasing evidence suggests that other cells and tissues are affected by the very low levels of SMN protein that cause the most severe forms of SMA.
The Parson Laboratory has previously identified that the structure of capillaries, which are the smallest blood vessels found in the body (Figure 1, see below), is severely affected in muscles and spinal cord of SMA mice and some people with the most severe forms of the condition. In the spinal cord, these blood vessel disruptions may contribute to an unfavourable environment for the motor neurons and thus have the potential to make SMA worse.
Dr. Allardyce has been further studying spinal cord post-mortem samples from severe, untreated people who had SMA, and looking very closely at the structure of the blood vessels.
Several key features of the vessels surrounding the motor neurons in the spinal cord were observed. Compared with unaffected controls, the SMA spinal cord had much smaller and abnormal-looking vessels, as well as an increase in the number of cells that line the inner surface of the blood vessels. In addition, more blood vessels were observed in the SMA spinal cord, suggesting that there is abnormal growth. There was also evidence of cellular damage, including swollen and ruptured cells with clear gaps between cells, which was linked with leakage of fluid out of the blood vessels.
A steady and efficient supply of blood to the spinal cord is required to maintain healthy neurons, including motor neurons. This important work reveals that blood vessel defects are likely to contribute to SMA in the most severe cases, and should be a target for future therapies.
Ilaria Signoria (University Medical Centre, Utrecht, Netherlands), a PhD student working with Ludo Van Der Pol and Ewout Groen, presented her work aiming to find out why there is a wide range of responses in the clinic to the SMN-dependent treatments of nusinersen and risdiplam.
On a population level, the more copies of SMN2 a person has, the less severe the SMA is likely to be. However, on an individual level, this is not always true; for example, people with SMA Type 2 may have two, three or four copies of SMN2. Similarly, when SMN-dependent treatments (e.g. nusinersen and risdiplam) are given to people with the same SMA Type and number of SMN2 gene copies, the effect on symptoms can differ between recipients.
Unfortunately, we do not currently know the reason for these difference between SMA subtypes and between treatment responses.
To provide some insight into this, Ms. Signoria grew skin cells that had been collected from 35 people with SMA (Types 1 to 4) and ten unaffected controls. Each SMA skin sample was taken from people with known SMN genetics and a detailed history of their condition. The skin cells, known as ‘fibroblasts’, are easily obtained, grow and multiply very quickly, and have the same genetic makeup as that of the donor; hence, they are a useful tool for assessing the impact of SMN-dependent therapies in the laboratory.
The skin cells from all 45 people were separately grown and assessed. The shape and size of all cells was evaluated, as were the levels of SMN protein. In addition, the intermediate molecule that is created from DNA to make a protein, known as ‘messenger RNA’, was also assessed. For more information on this, click here.
There were no clear differences in the shape and size of the skin cells from people with SMA compared to controls. However, as expected, there were reductions in the SMN protein and the ‘messenger RNA’ from the SMN1 and SMN2 genes in the SMA ‘fibroblasts’.
Skin cells taken from people with more SMN2 copies generally had higher availability of SMN protein and ‘messenger RNA’. Furthermore, those cells with more SMN2 copies tended to produce more SMN protein when treated with the SMN2-targeting therapies nusinersen and risdiplam.
Interestingly, it was found that the levels of SMN ‘messenger RNA’ did not correlate well with the amount of SMN protein, suggesting that factors involved in converting the ‘messenger RNA’ into protein differ between individuals, and that the process can be more efficient in some people than others.
It was also observed that factors such as age, SMN2 copy number and SMN levels before treatment were only able to explain a proportion of the variability in response to the treatments. This suggests that other currently unknown factors are at play.
The ‘fibroblast’ model is a powerful tool to identify what these factors are. This is exciting because, in the future, we may be able to manipulate these factors in people with SMA to improve individual responses to the SMN-dependent therapies.
Saman Rashid (University of Hertfordshire, UK), a PhD student in the laboratory of Maria Dimitriadi, presented his work using the microscopic organism known as C. elegans (Figure 2, see below).
C. elegans is a small worm often used in research because it is inexpensive to work with, very quick to breed, and it shares many of genes and cellular processes with humans. This worm has a very similar SMN protein to us, and has therefore been used in many laboratories around the world to provide important insights into the cellular function of the SMN protein.
‘Autophagy’ is a critical process that occurs within cells to recycle and remove bi-products of metabolism, as well as other unwanted substances. When it goes wrong, these substances can accumulate and impair the health of cells and tissues. Defects in ‘autophagy’ have been linked to several nervous system diseases, including SMA.
Mr. Rashid has been working with a worm model of SMA that has low levels of the SMN protein and displays neuromuscular defects with a shortened lifespan. He first reported that SMA worms display signs that ‘autophagy’ is overly active, which could be contributing to disease in this model.
With this in mind, Mr. Rashid performed a small scale screen of drugs able to modify various steps of in ‘autophagy’ process. After treating SMA worms with these drugs, he assessed the impact on neuromuscular function. A drug called fluphenazine was identified to improve the movement and feeding behaviour of SMA worms. Fluphenazine was also shown to increase lifespan, all without altering SMN protein levels.
This interesting work identifies that impaired ‘autophagy’ may be contributing to SMA, and that enhancing the process with drugs could provide a possible SMN-independent treatment approach. However, further work is needed to fully understand exactly how the drugs targeting ‘autophagy’ are able to improve the SMA worms.
The work also highlights the importance of using a range of animal models to study SMA and how re-purposing already approved drugs could be of benefit to nervous system diseases.
Scott Baver (Scholar Rock, Cambridge, USA), a Vice President at Scholar Rock, provided an update on the TOPAZ trial of apitegromab.
TOPAZ is an ongoing phase 2 study designed to assess the safety and efficacy of apitegromab administered in conjunction with nusinersen or risdiplam. Trial participants are non-ambulatory (unable to walk independently) and aged 2-21 years living with SMA Type 2 or Type 3 (click here for more information).
Dr. Baver presented the latest data from the trial on the impact of apitegromab after 36 months of treatment. Of the 57 participants enrolled in the extension part of TOPAZ, six discontinued their involvement due to COVID-19-related concerns, perceived lack of benefit or scheduling issues.
In the remaining 51 participants, motor function is being assessed using the standard scales of the Hammersmith Functional Motor Scale – Expanded (HFMSE) and Revised Upper Limb Module (RULM).
After 36 months, sustained improvements in motor function were reported, with 86% of people improving upon or maintaining World Health Organisation (WHO) motor milestones that they had achieved at baseline. In addition, participant- and caregiver-assessment of daily activities, mobility and fatigue indicated self-reported, sustained improvements over the 36 month period.
Apitegromab continues to be safe and well-tolerated, and these intermediate results support the continued assessment of the drug for the treatment of SMA. Participants will be treated and monitored until 48 months, the results of which will be reported in due course.
Martin Skov (NMD Pharma, Aarhus, Denmark), innovation manager at NMD Pharma, presented data from a trial of a new, investigational drug called NMD670 with potential for SMA.
NMD670 is an orally-bioavailable, small molecule that specifically targets a protein called ClC-1 that is found almost exclusively on the surface of muscles cells. The function of ClC-1 is to dampen the excitability of muscles and prevent them from becoming overstimulated.
By inhibiting ClC-1 function, NMD670 can increase and improve the passage of signals from motor neurons to muscles, which can increase how easily muscles are able to contract. NMD670 therefore has potential for the treatment of SMA, where the passage of electrical signals from motor neurons to muscles can be severely affected.
Dr. Skov presented work using a rat model of a neuromuscular disease called myasthenia gravis. The data indicate that single and prolonged administration of NMD670 can improve muscle function and mobility of the model. In addition, NMD670 was also tested in 12 people with myasthenia gravis and shown to be safe and cause clinically meaningful improvements in the disease.
Given that NMD670 improves muscle function, it was hypothesised that it could be valuable for the treatment of SMA. Hence, experiments were performed showing that NMD670 was capable of improving the electrical signalling between motor nerves and muscles in a mouse model of SMA, leading to a marked increase in muscle strength.
Given these results, the SYNPASE-SMA trial of NMD670 was initiated in late 2023 in North America and Europe. Designed to assess the efficacy, safety, and tolerability of NMD670 in 50 ambulatory participants with SMA Type 3, SYNPASE-SMA is a phase 2, randomized, double-blind, placebo-controlled study.
SYNPASE-SMA is estimated to be completed in late 2024, and the findings will be published and publicised in due course.
To read more about NMD670, see:
Leandra Ros (University Medical Centre, Utrecht, Netherlands), a PhD student and medic working with Ludo Van Der Pol and Renske Wadman, presented work that assessed the impact of the cold on SMA symptoms.
Cold temperatures can affect muscle performance and there are many personal reports that muscle weakness is temporarily aggravated in SMA during exposure to the cold – a phenomenon known as ‘cold paresis’. However, the presence of temperature-induced symptoms in SMA, for example weakness and fatigue, has not been systematically evaluated in a clinical setting – until now.
Dr. Ros and colleagues designed a questionnaire to assess the frequency and severity of cold-induced symptoms in 103 adolescents and adults with SMA Types 1 to 4, who had not received any SMN-targeting therapies. 80% of participants were unable to walk, while the rest were ambulant.
25 age-matched, unaffected individuals were used as a control group, and no cold-induced symptoms were reported in this cohort.
On the contrary, cold-induced symptoms were reported by 87% of people with SMA; these included weakness (85% of people), fatigue (29%) numbness (20%), pain (16%) and tingling (15%). Participants with SMA Type 1 and 2 all reported cold-induced weakness, while only 35% of ambulant participants suffered from the cold.
Using the HFMSE and RULM motor scales, a correlation between motor function and ‘cold paresis’ was identified in non-walkers, but not ambulant participants. Moreover, disease severity, but not age or disease duration, appears to be the main factor in the development of cold-induced weakness.
This study confirms that cold-induced weakness and additional difficulties are a prevalent and important symptom that is experienced by most people with SMA, especially those with more severe types. This improved understanding of cold paresis is the first important step towards identifying its causes, with a view to developing appropriate treatment strategies in the future.